
What is GLP-1? The Complete Guide to the Hormone Behind Modern Weight Loss
Key takeaways
- GLP-1 is made by intestinal L-cells when you eat.
- It controls insulin, gastric emptying, and appetite at once.
- Ozempic and Wegovy are synthetic GLP-1 receptor agonists.
- Fiber, butyrate, allulose, and protein all boost natural GLP-1.
- Natural boosters work slower than the drugs but with fewer side effects.
GLP-1 (glucagon-like peptide-1) is a hormone made in the gut that lowers blood sugar, slows stomach emptying, and reduces appetite. Prescription drugs like Ozempic and Wegovy work by mimicking this hormone. You can also raise your body's own GLP-1 through fiber-rich foods, butyrate-producing gut bacteria, protein, and specific supplements.
If you've heard about Ozempic, Wegovy, Mounjaro, or Zepbound in the last 2 years, you've heard about GLP-1. The drugs themselves are everywhere. The hormone they're built around is mostly a mystery to people outside research medicine. This guide is the plain-English version.
We're going to walk through what GLP-1 actually is, how your body makes it, why pharma companies built a 100-billion-dollar weight-loss category around it, and what's realistic to expect if you want to raise your own GLP-1 without a prescription.
What is GLP-1, in plain English?
GLP-1 stands for glucagon-like peptide-1. It's a peptide hormone, meaning a small protein your body makes to send messages between organs.
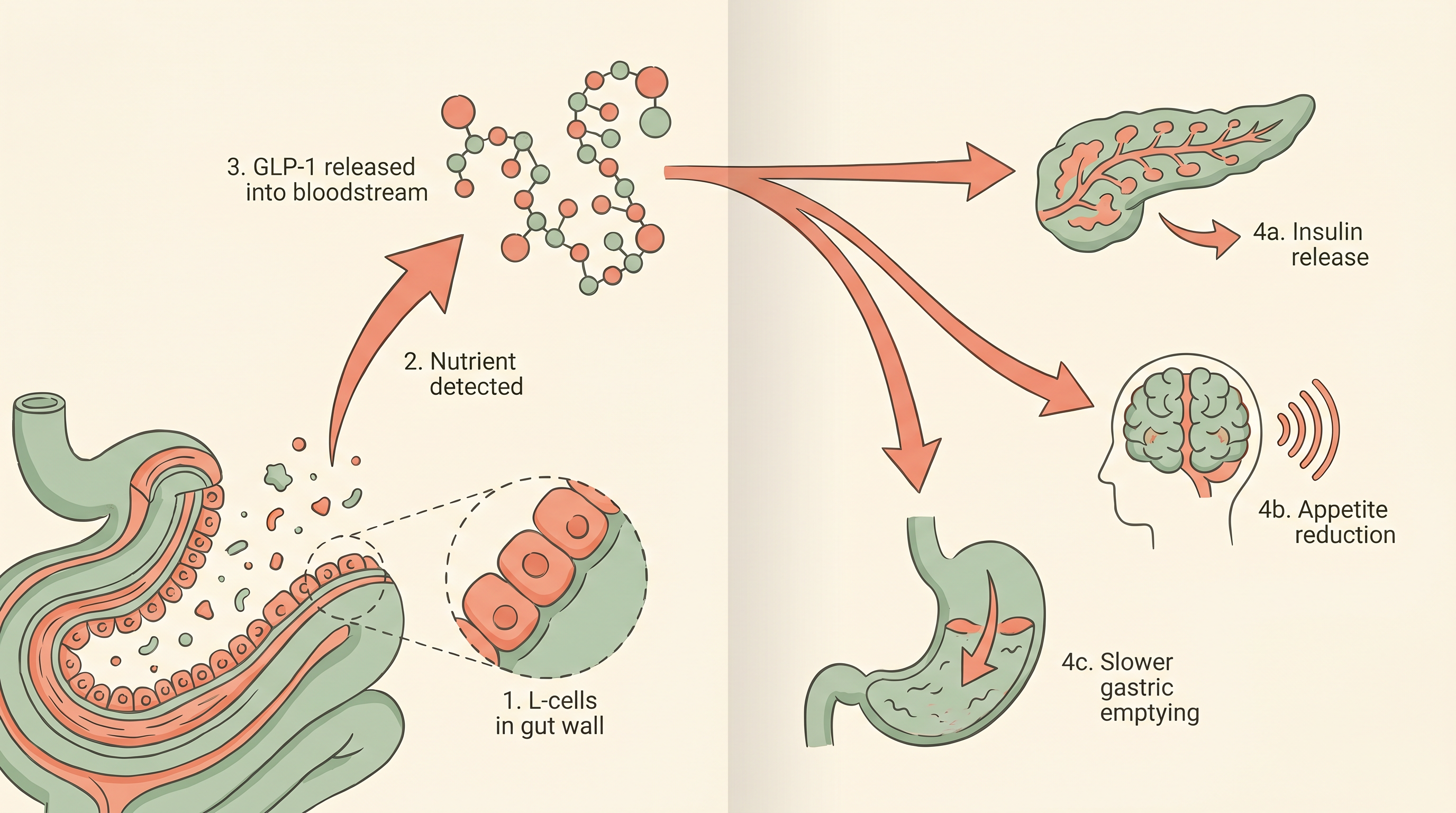
Specific cells in the lining of your small intestine, called L-cells, release GLP-1 within minutes of food entering your gut (Drucker 2018). Once released, GLP-1 travels through your bloodstream and acts on three different organs almost simultaneously: the pancreas, the stomach, and the brain.
The pancreas reads the signal and releases insulin. The stomach slows its rate of emptying. The brain registers fullness and ramps down hunger. That triple-action effect is what makes GLP-1 such an unusual hormone, and why it became the foundation of an entire class of weight-loss drugs.
For decades, GLP-1 was a research curiosity. Then someone figured out how to make a synthetic version that hangs around in the body long enough to actually work as a medication. That synthetic version became semaglutide (Ozempic, Wegovy), liraglutide (Saxenda), tirzepatide (Mounjaro, Zepbound), and a half-dozen others now in trials.
How does your body release GLP-1?
The release pathway is straightforward but worth understanding because it explains why some foods and supplements work better than others at raising GLP-1.
Step one: you eat something. Step two: as the food moves into your small intestine, it makes contact with L-cells embedded in the gut lining. L-cells have receptors that sense specific nutrients, particularly short-chain fatty acids, certain amino acids, glucose, and fats (Holst 2007).
Step three: those L-cells release stored GLP-1 into the bloodstream. Step four: the hormone reaches the pancreas, the stomach, and the brain within minutes, and starts doing its three jobs.
Here's the catch: GLP-1 has an extremely short half-life. About 2 minutes, by most measurements (Müller et al. 2019). An enzyme called DPP-4 chews it up almost as fast as L-cells make it. So even when your body releases plenty of GLP-1, the effect doesn't last long. That's the problem prescription GLP-1 drugs solve by being chemically resistant to DPP-4.
For someone trying to raise GLP-1 naturally, the takeaway is different: you can't store it up. You support it through consistent meals, gut bacteria that keep producing GLP-1-stimulating short-chain fatty acids, and habits that keep your body in a steady release pattern rather than a single huge burst.
Why is GLP-1 the hormone behind modern weight loss?
Because almost no other hormone hits all three of the levers that drive weight at once.
Most weight-loss approaches focus on a single lever. Calorie restriction targets intake. Exercise targets expenditure. Appetite suppressants target hunger. Insulin sensitizers target blood sugar. GLP-1 turns out to hit all four at the same time.
Clinical evidence stacked up fast. The STEP-1 trial of semaglutide showed an average 14.9% body weight loss in 68 weeks (Wilding et al. 2021). The SURPASS-2 trial of tirzepatide showed up to 22.5% weight loss at the highest dose (Jastreboff et al. 2022). Those numbers are unlike anything any pill or behavioral intervention had ever produced in a similar timeframe.
No other hormone hits all three weight levers at once. That's the entire reason GLP-1 became a category.
Beyond weight, GLP-1 also has direct benefits on cardiovascular outcomes (Marso et al. 2016) and emerging signals on dementia, addiction, and inflammation. The story is still being written, but the metabolic story is now well-established.
That said, the drugs have real downsides: nausea, vomiting, GI distress, muscle loss, gallstones in some patients, and a 70% one-year discontinuation rate in real-world cohorts (Gleason et al. 2024). Weight tends to come back after stopping. The cost is also significant: $1,000 to $1,500 per month out of pocket without insurance coverage. Those gaps are what's driving interest in natural alternatives.
What's the difference between prescription GLP-1 drugs and natural boosters?
The simplest way to think about it: prescription drugs supply synthetic GLP-1 directly. Natural boosters help your own body make and use more GLP-1 it already produces.
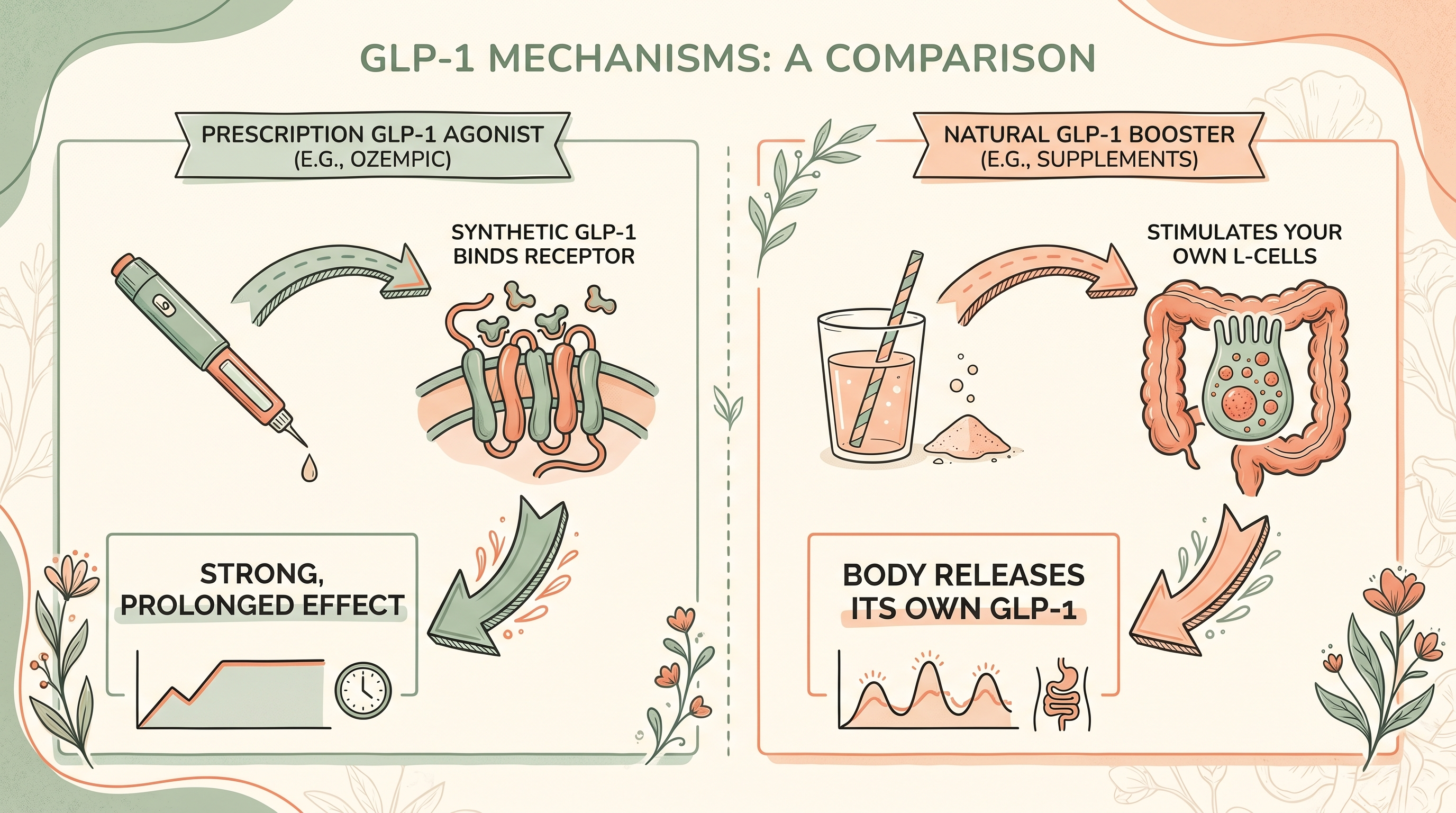
The size of the effect is different. Prescription semaglutide produces a GLP-1 level 10 to 50 times higher than your body would naturally hit after a meal, and keeps it there for a week per injection (Müller et al. 2019). Natural boosters produce smaller increases for shorter windows.
The side effect profile is also different. Prescription drugs work fast but commonly cause nausea, diarrhea, constipation, and food aversion strong enough to feel like illness. Natural boosters work more gradually, with most people reporting reduced appetite and cravings rather than dramatic side effects.
The lifestyle commitment is different too. A weekly injection plus monitoring vs. drinking a stick pack in water once a day, or eating more fiber, or taking a supplement. Most people find the natural route easier to stick with for a year. The drugs produce more impressive short-term results.
How can you increase GLP-1 naturally?
Seven approaches have peer-reviewed human data behind them. They're not exotic, and most of them stack.
| Strategy | Mechanism | Evidence |
|---|---|---|
| High-protein meals | Amino acids directly stimulate L-cells | Strong, multiple human trials |
| Soluble fiber (psyllium, glucomannan, inulin) | Slows digestion; ferments to short-chain fatty acids that trigger L-cells | Strong |
| Butyrate or butyrate-producing prebiotics | Directly activates FFAR receptors on L-cells | Strong (preclinical and clinical) |
| Allulose | Rare sugar that triggers GLP-1 release without raising blood glucose | Moderate (Japanese clinical trials) |
| Healthy fats (olive oil, nuts) | Fatty acids stimulate L-cells via FFAR1 | Moderate |
| Exercise | Acute and chronic increases in postprandial GLP-1 | Moderate |
| Berberine | Stimulates GLP-1 release via AMPK pathway | Strong (rivals metformin in head-to-head) |
For more on which supplements stack best, see our guide to supplements that curb sugar cravings. For ingredient-specific deep-dives, we've also covered whether allulose causes bloating and foods that boost gut butyrate production.
How does the gut-brain axis fit into all this?
GLP-1 is one of the major messengers in what researchers call the gut-brain axis: the constant chemical and electrical conversation between your digestive tract and your central nervous system.
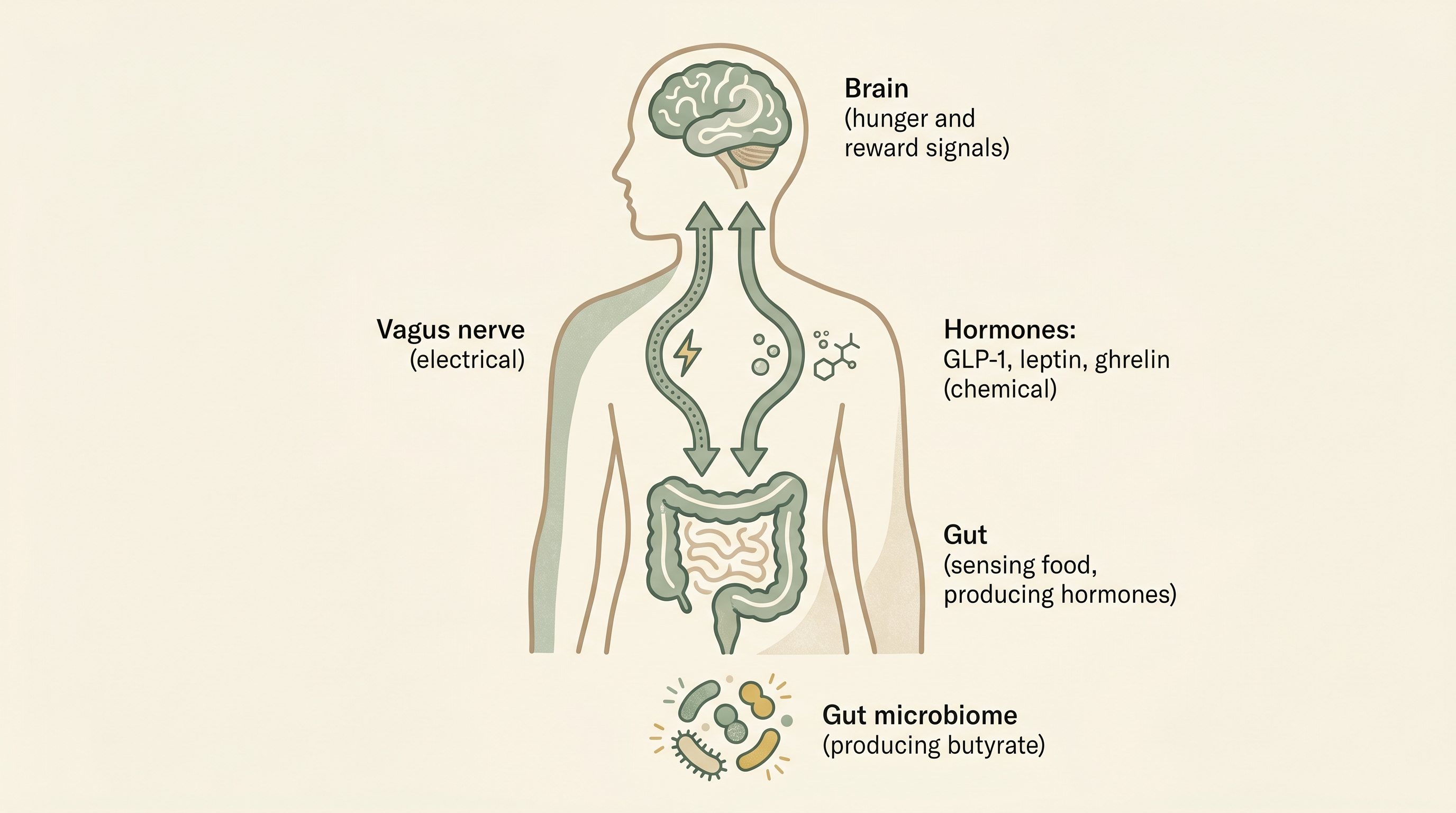
The vagus nerve carries electrical signals from gut to brain in milliseconds. Hormones like GLP-1, leptin, ghrelin, and PYY carry chemical signals through the bloodstream in minutes. Both pathways converge on the hypothalamus, where decisions about hunger, fullness, and food reward get made (Mayer 2011).
Your gut microbiome plays a major role here. Specific bacteria ferment dietary fiber into short-chain fatty acids, especially butyrate, acetate, and propionate. Those short-chain fatty acids both stimulate GLP-1 release directly and reinforce L-cell health over time (Cryan et al. 2019). That's why diet and gut health track so closely with appetite regulation.
This is the basis for why ingredients like L-lysine butyrate, inulin, and chicory root keep showing up in newer GLP-1 booster products. They feed the system that makes the hormone.
Are natural GLP-1 boosters actually effective?
Yes, but the question is what "effective" means in context.
For postprandial GLP-1 response (how much GLP-1 you make after a meal), natural strategies measurably increase the response. Whey protein increases postprandial GLP-1 by 50 to 100% compared to a control meal (Adams et al. 2015). Psyllium increases it. So do berberine, allulose, and butyrate stacks.
For weight loss specifically, the gap with prescription drugs is real. Semaglutide produces 15% body weight loss in a year. The best natural-supplement clinical trials show 2 to 6% over the same period. The drugs are simply more potent in this metric, though that potency comes with discontinuation rates and rebound weight regain.
For appetite and craving reduction, the gap is smaller. Multi-ingredient blends, fiber stacks, and protein-forward eating produce subjective craving reductions that many users describe as similar to "Ozempic-lite" without the nausea. Food noise, that constant mental chatter about food, often drops within days for supplement stack users.
The drugs are more potent. Natural approaches are easier to sustain and rarely cause side effects worth worrying about.
The honest pitch for natural GLP-1 boosters is: smaller effect, lower side-effect burden, much cheaper, sustainable for years rather than months. The honest pitch for the drugs is: bigger effect, faster, with significant downsides and a high failure-to-maintain rate.
Who shouldn't try to raise their GLP-1?
Most healthy adults can safely target higher natural GLP-1. A few groups should be careful or talk to a clinician first.
People with gastroparesis or significant GI motility issues. GLP-1 slows gastric emptying. If your stomach already empties too slowly, more delay can worsen symptoms.
People on certain diabetes medications. Combining strong natural GLP-1 boosters with insulin or sulfonylureas can theoretically cause hypoglycemia. Coordinate with the prescriber.
People with a personal or family history of medullary thyroid carcinoma or MEN2. This is a labeled contraindication for prescription GLP-1 drugs based on rodent data. Translating that caution to natural boosters is overcautious in most cases, but worth a doctor's review.
Pregnant or breastfeeding women. The data on GLP-1-boosting supplements during pregnancy is limited. Default to caution.
For someone transitioning off a prescription GLP-1, natural boosters are often the bridge that prevents rebound hunger. That's one of the highest-leverage use cases.
The bottom line: who is GLP-1 actually for?
GLP-1 isn't a niche hormone for diabetics. It's a central metabolic regulator that everyone has, working around the clock to coordinate digestion, blood sugar, and appetite. The interesting question isn't whether you have GLP-1. You do. It's whether you're supporting it well.
Three groups benefit most from paying attention.
People who want to lose weight without prescription drugs. Diet, protein, fiber, gut support, and possibly a multi-ingredient GLP-1 blend cover most of what the drugs do, at a smaller effect size.
People who tried Ozempic or Wegovy and stopped. Hunger returns within weeks of stopping a prescription GLP-1. Natural support is the easiest off-ramp.
People with metabolic markers drifting. Pre-diabetes, rising A1C, persistent post-meal energy crashes. Boosting natural GLP-1 response is one of the highest-leverage moves before things require medication.
This is the topic that pulls almost everything else on the Ozzi blog together. If you only read one piece to understand the science behind cravings, weight, blood sugar, and the new wave of metabolic medications, this is the one.
Frequently asked questions
What does GLP-1 stand for?
GLP-1 stands for glucagon-like peptide-1. It's a peptide hormone made in the lining of your small intestine.
How long does natural GLP-1 last in the body?
About 1 to 2 minutes. An enzyme called DPP-4 breaks GLP-1 down very quickly.
What foods naturally boost GLP-1?
High-protein foods, soluble fiber from oats and beans and psyllium, butyrate-producing prebiotics, healthy fats, and the rare sugar allulose.
Is Ozempic the same as GLP-1?
No. Ozempic (semaglutide) is a synthetic drug that mimics GLP-1.
Can you take a supplement to raise GLP-1?
Yes. Berberine, glucomannan, allulose, L-lysine butyrate, chicory inulin, and African mango extract all have peer-reviewed evidence.
Do natural GLP-1 boosters cause side effects?
Most don't. Berberine can cause GI upset and glucomannan needs water.
How long until I notice a difference with natural GLP-1 support?
Most people report reduced cravings within 3 to 7 days. Weight effects build over 4 to 12 weeks.
Is GLP-1 the same as insulin?
No. GLP-1 tells the pancreas to release insulin when needed.
References
- Drucker DJ. Mechanisms of action and therapeutic application of glucagon-like peptide-1. Cell Metab. 2018;27(4):740-756. PubMed
- Holst JJ. The physiology of glucagon-like peptide 1. Physiol Rev. 2007;87(4):1409-1439. PubMed
- Müller TD, Finan B, Bloom SR, et al. Glucagon-like peptide 1 (GLP-1). Mol Metab. 2019;30:72-130. PubMed
- Wilding JPH, Batterham RL, Calanna S, et al. Once-weekly semaglutide in adults with overweight or obesity (STEP 1). N Engl J Med. 2021;384(11):989-1002. PubMed
- Jastreboff AM, Aronne LJ, Ahmad NN, et al. Tirzepatide once weekly for the treatment of obesity (SURMOUNT-1). N Engl J Med. 2022;387(3):205-216. PubMed
- Marso SP, Daniels GH, Brown-Frandsen K, et al. Liraglutide and cardiovascular outcomes in type 2 diabetes (LEADER). N Engl J Med. 2016;375(4):311-322. PubMed
- Gleason PP, Urick BY, Marshall LZ, et al. Real-world persistence and adherence to GLP-1 receptor agonists. J Manag Care Spec Pharm. 2024;30(8):860-867. PubMed
- Mayer EA. Gut feelings: the emerging biology of gut-brain communication. Nat Rev Neurosci. 2011;12(8):453-466. PubMed
- Cryan JF, O'Riordan KJ, Cowan CSM, et al. The microbiota-gut-brain axis. Physiol Rev. 2019;99(4):1877-2013. PubMed
- Adams RL, Broughton KS. Insulinotropic effects of whey. Ann Nutr Metab. 2015;69(1):56-63. PubMed
- Yin J, Xing H, Ye J. Efficacy of berberine in patients with type 2 diabetes mellitus. Metabolism. 2008;57(5):712-717. PubMed
- Iwasaki Y, et al. GLP-1 release and vagal afferent activation mediate the beneficial metabolic effects of D-allulose. Nat Commun. 2018;9(1):113. PubMed
Want to support your natural GLP-1 without a prescription?
Ozzi Crave Crusher combines L-lysine butyrate, glucomannan, chicory inulin, allulose, African mango extract, and chromium into a single drink stick. Six mechanisms, one serving. Use it for 10 days. If you don't feel a difference, we'll refund your first bag.